3 Steps for Reducing Costs and Errors in Clinical Trials
Clinical trial costs are trending upward, driven by a variety of factors, such as increasing trial complexity and rising travel costs for training, meetings and monitoring. While some of these factors are largely fixed, costs can be controlled by focusing on areas that lie well within the sponsors’ and research sites’ control.
And much of that focus should be on things that can lead to errors, which can significantly increase the time needed to complete a clinical trial, require work to be re-done and require corrective actions, such as staff re-training, that also add to costs.
But three simple steps can help clinical researchers reduce both errors and costs during studies. The trick is to focus on those parts of clinical trial preparation and conduct that can most affect key drivers of cost increases.
Clinical trials are expensive. There is no way of getting around that fact. AMarch 2022 blog on the My Onsite Healthcare website estimated that the cost of bringing a new drug to market runs between $161 million and $2.6 billion. This can translate to an average cost of $41,000 per patient, according to a 2019 article in Clinical Leader.
Myriad factors go into the cost of a clinical trial. The costs to manufacture, transport and store the investigational product, for instance, are important and immutable. Staff salaries, travel costs and the cost of equipment and supplies can also play a role. But some factors have a greater impact than others.
Errors in enacting the protocol can add significantly to the cost of a clinical trial, primarily by adding time and person-hours, as well as requiring work to be repeated for errors egregious enough to threaten the validity of data gathered.
And protocol deviations or errors are common. According to FDA data, protocol deviations remained the top BIMO inspection observation for 2021, as they have for the last several years.
The Tufts Center for the Study of Drug Development (CSDD) agreed, noting in >an early 2022 reportthat the mean number of protocol deviations and substantial amendments—another cost and time driver—have increased across all clinical trial phases. The typical Phase 3 trial has 119 deviations, the CSDD report said.
Amendments are particularly troublesome. The timeline for protocols with three or more substantial amendments tend to require nearly three more weeks of treatment for enrolled patients and see close-out delayed by nearly four weeks, the CSDD estimated.
Step 1: More complex trials call for clearly written protocols
Recent attention has focused on growing clinical trial complexity as a cost driver. More complex trials tend to take longer, which adds to the cost of a study. More complex protocols also tend to offer more opportunities for errors, which can add additional time and expense to correcting those errors.
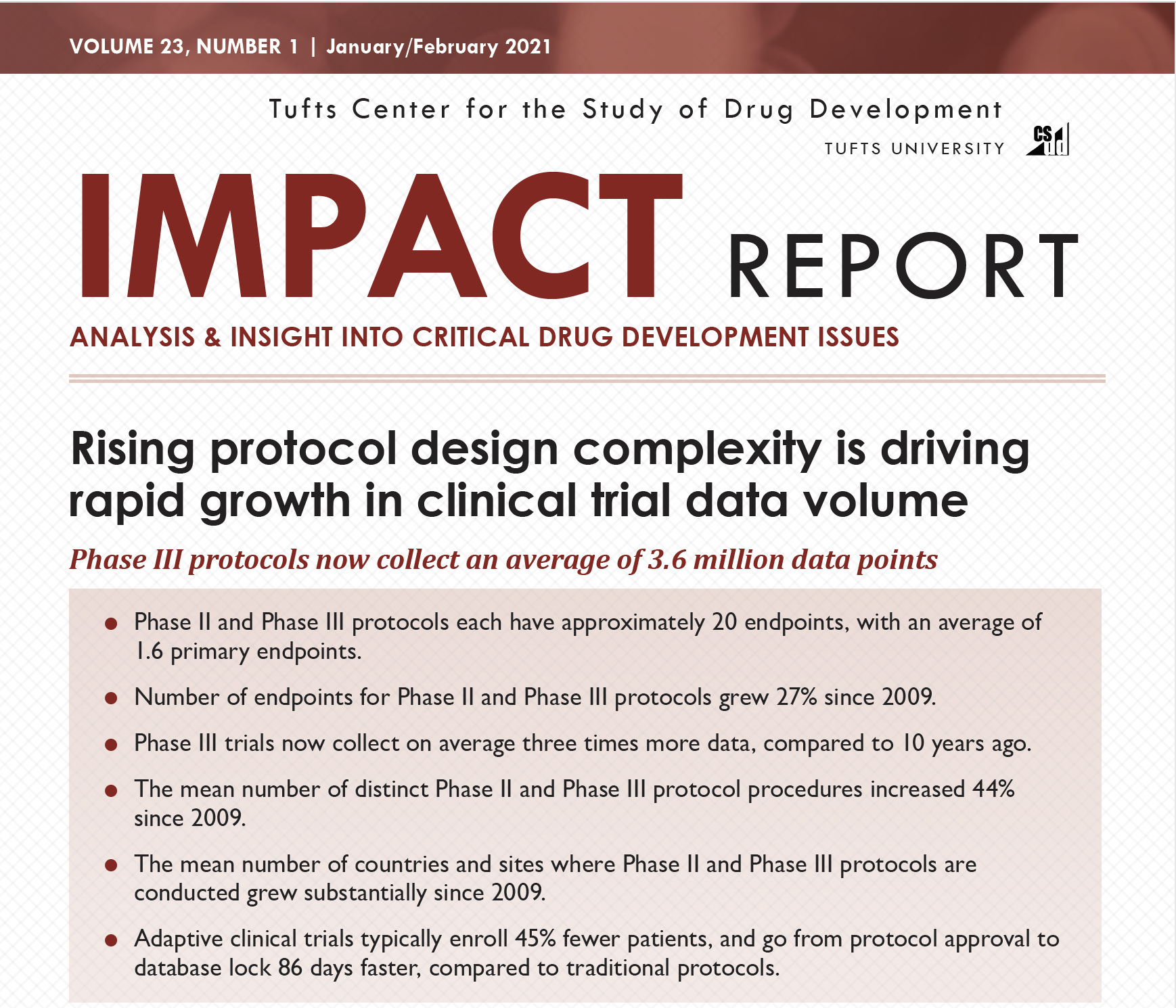
A 2021 study by the Tufts Center for the Study of Drug Development (CSDD) noted that protocols have been growing increasingly complex since 2009, with no end in sight to that trend. For instance, the CSDD report said that Phase II and III protocols as of 2020 generally had about 20 endpoints, with an average of 1.6 primary endpoints, up 27% since 2009. And the mean number of distinct procedures required for a typical protocol rose 44% during the same timeframe.
So, the first step to cost control is to focus on the protocol, ensuring that it is written in a way that is clear and easy to understand, both across sites and across jobs at any given site. As noted above, the growing complexity of clinical trials has been tagged by experts as one of the top reasons for protocol deviations or errors to occur. Protocols that include many individual procedures, require novel procedures that differ from standard of care and/or have a larger number of endpoints can be particularly prone to errors.
Including site staff early in protocol development can help ensure that protocols are written in a way that is clear to all employees. For larger trials that involve global sites, consideration of how language and cultural differences may impact protocol adherence is also important. And site resources and expertise also need to be considered when developing a protocol; not all sites will have access to the same equipment and supplies or have the same levels of expertise in all areas.
Step 2: Training to ensure predictable performance
The next step then must be to provide thorough, effective training designed to ensure that all staff fully understand how to do their jobs in line with the protocol. And this can be challenging to achieve with a traditional lecture- or slide-based training session.
In 2019, Harvard indicated that slide-based training and education is not effective in imparting knowledge in a way that alters performance, calling the combination of slides and lecture “worse than useless.” This is important for clinical research applications because the entire purpose of training on a protocol is to ensure that behavior is changed for the better—“better” meaning accurately carrying out tasks as described in the protocol.
For example, failure to correctly apply inclusion and exclusion criteria during patient screening can lead to a mismatch in patients and the protocol. The end result of this is likely time and money spent collecting data that ultimately cannot be used as part of an application for new product approval.
Examples of the value of simulation can be found in other industries, such as aviation, where crashes are greatly reduced when pilots are trained via simulation. Similarly, within the healthcare industry, simulation training has been used to reduce anesthesia mishaps.
Protocol simulation training provides actual practice in critical study skills, including GCPs, pharmacokinetics, informed consent, placebo arms and investigational product handling, among others.
An important feature of simulation-based training is the ability to identify and focus on weak areas, while also predicting staff and site performance before a study even begins. Simulation training provided by Pro-ficiency, for example, includes a dashboard that highlights how staff within a site performs during training, as well as performance across multiple sites. Sponsors can quickly identify where protocol procedures have been mastered, where significant knowledge gaps exist and where some corrective guidance was needed during the training process.
This lets sponsors quickly and easily identify poor-performing sites and individuals, as well as narrowing down where weaknesses exist. This allows for additional, closely targeted training and support before the first patient is enrolled in a trial, which helps to avoid errors and associated costs during the study.
This type of feedback can also quickly identify any problem metrics showing that most people struggle with a particular task or procedure. This knowledge can be applied to improve the way the protocol is written, if necessary, further reducing costs by going back to ensuring the protocol is clear.
Equally important is the ability to identify “heroes” at individual sites, as well as “rock star” sites, that who perform exceptionally well.
Step 3: Decision support tools to aid long-term performance
The final step is closely linked to the training. It is not at all uncommon for training to occur well before sites begin enrolling patients. This lag in time between learning protocol procedures and having to apply them can lead to less reliable recall, which can cause errors and up costs.
Decision support tools can be developed alongside a simulation-based training program to provide site employees with references that they can use once a clinical trial is underway. For example, tools to aid research coordinators and investigators in patient screening could list inclusion and exclusion criteria; the availability of simple lists of this sort can help to reactivate the “muscle memory” generated with the simulations included in training.
Novel or complex procedures required for a given protocol could likewise be supported with checklists and/or illustrations. Decision support tools provided in an electronic format could even include brief animations that employees could reference to remind them of the correct way of completing the procedures. For instance, if a special sort of imaging is required for a study, a support tool could list key steps and identify ways in which the protocol’s imaging procedures differ from standard practice.
Decision support tools can be provided in hard copy form, such as checklists, flow charts or flash cards, or in electronic form that can be accessed with a tablet, phone or through a site’s computer system.
Errors and protocol deviations are among the top factors that add to a clinical trial’s time and costs. As with many problems, proactively identifying and addressing potential errors is more effective and cost-efficient than merely reacting after an error occurs. By focusing first on writing a clear and easily understandable protocol and second on providing effective training and related decision support tools to site staff, sponsors can help assure that they address potential errors up front and reduce the likelihood that deviations will increase the time and cost needed to complete their clinical trials.
To learn more regarding how to reduce clinical trial costs, visit our website: http://proficiency1.wpenginepowered.com/

Dave Hadden is an entrepreneur and technology innovator, founding Pro-ficiency and pioneering the fields of A.I.-based medical decision-support, Training Analytics, and Virtual Patient Simulation (VPS). Dave has focused his passion for technological innovation and learning systems in the field of clinical trials, helping sponsors make their studies more accurate and efficient through finding the right technology mix such as virtualization, performance management and applied behavioral sciences to produce the most effective, lasting, and engaging results for clinical trials.


{kind=link}
{kind=link}
Comments are closed.